

A sinus lift rebuilds bone in the upper jaw so a dental implant has a solid base — the surgery itself takes only one to two hours, but recovery is the long part: the grafted area usually needs around six to nine months to fully integrate before the implant goes in. Here’s how the procedure actually works, the real stage-by-stage healing timeline, where stem cells fit, and the risks worth understanding before you commit.
If you’re not yet sure whether you even need one, start with how to tell if you need a sinus lift for dental implants. This guide assumes you do, and focuses on what to expect from the procedure and the months that follow.
What Happens During a Sinus Lift
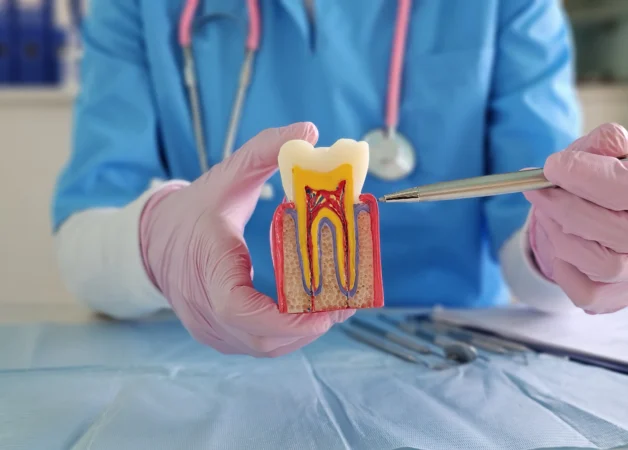
It sounds complex, but the procedure itself is fairly straightforward. It rebuilds bone height in the upper jaw, near the back teeth, where the sinus cavity often sits too low to leave room for an implant. The steps run like this:
- Access. A small incision exposes the jawbone, and a window is opened in the lateral wall of the sinus to reach the membrane.
- The lift. The sinus membrane is gently lifted upward to create space beneath it.
- Graft placement. Bone graft material is packed into that space.
- Closure. A protective membrane is placed over the graft, and the gum is sutured closed to heal.
Two things worth knowing up front. It isn’t for everyone — a sinus lift is typically indicated when upper-jaw bone height is too low for a stable implant (often below roughly 5 mm). And while the surgery takes only one to two hours, the healing is the long part, which is the next section. The graft material itself is the same family used in a standard bone graft for dental implants.
Sinus Lift Recovery: The Healing Timeline, Stage by Stage
Bone doesn’t form all at once — it follows a biological sequence, and understanding it explains why the wait is unavoidable.
- Inflammation & clot (first days to a week). The site is vulnerable; the body sends healing cells and forms a protective clot over the graft.
- Soft-tissue formation (weeks 2–3). Soft tissue closes the wound and shields the graft underneath.
- Early bone integration (weeks 4–6). Bone-forming cells begin laying down new bone. The area is still fragile, so hard or crunchy foods are off the menu.
- Maturation & remodelling (month 2 onward, up to 6–9 months or more). The graft properly bonds with living bone — the stage that decides whether the foundation holds, and the one you can’t rush.
During recovery, avoid anything that pressurises the sinus — try not to blow your nose forcefully, and sneeze with your mouth open — until your surgeon clears you.
Where Stem Cells Fit In
The long healing window is what makes regenerative approaches appealing, and stem cell therapy draws the most interest for sinus augmentation. The idea is to enhance the body’s own bone-building rather than replace the graft: mesenchymal stem cells (MSCs) — from bone marrow, fat or dental pulp — are applied to the graft site, where they can develop into bone-forming cells, potentially speeding regeneration, improving blood supply and helping the graft integrate.
Here’s the honest framing. Early clinical evidence suggests MSCs used alongside graft material can support new bone growth and better vascularisation³⁴ — but the keyword is alongside. Reviews of human trials consistently conclude cell-based therapies work as an adjunct to grafting, not a replacement, and that there still isn’t enough evidence to identify the best technique.³ They’re also offered at only a limited number of clinics, as approval varies by country. The proven foundation is still the graft itself, planned and placed well — the same conclusion reached in our wider guide to rebuilding lost jawbone.
Risks and Complications Worth Understanding
Sinus lifts are safe and routine, but no surgery is risk-free, and a good clinic is upfront about that.
- Sinus membrane perforation — the most common complication; across studies it occurs in roughly a quarter of cases.¹ Reassuringly, when detected and repaired during surgery it does not appear to reduce long-term implant survival.¹² Careful technique and tools like piezoelectric instruments lower the risk.¹
- Sinus infection — possible while the site heals; signs include pain, fever and nasal discharge. Most cases are controlled with antibiotics.
- Graft failure — when the graft doesn’t produce enough new bone; re-grafting is done once the area has healed.
The thread running through all of these: outcomes depend heavily on the surgeon’s experience and planning. This is a procedure where who does it, and how carefully they plan it, genuinely matters.
Frequently asked questions
How long is recovery after a sinus lift?
Is a sinus lift painful?
What should I avoid after a sinus lift?
What happens if the sinus membrane tears?
Why Patients Choose DentSpa for Sinus Lifts and Implant Preparation
A sinus lift is, above all, a planning-and-skill procedure — and that’s where DentSpa concentrates. The clinic uses 3D CBCT imaging to map sinus anatomy, membrane position and bone volume before surgery, so the lift and graft are planned precisely rather than judged on the day, with careful technique to minimise complications.
It also handles everything the sinus lift leads to — single implants, implants for multiple teeth, and full-arch All-on-4 and All-on-6 — and aftercare continues remotely once you’re home, with records shareable with your local dentist during the long healing phase. Recognised as the Best Clinic in Dentistry in Europe at the European Awards in Medicine 2024 and trusted by 50,000+ international patients, DentSpa gives you a realistic plan and timeline up front. Book a free consultation and send recent X-rays or a scan to get started.
Sources
- Incidence, risk factors and complications of Schneiderian membrane perforation in sinus lift surgery: a meta-analysis. Int J Oral Maxillofac Implants. 2016. https://pubmed.ncbi.nlm.nih.gov/26974034/
- Management of Schneiderian membrane perforations during sinus floor augmentation and subsequent implant survival: a systematic review and meta-analysis. Int J Implant Dent. 2021. https://link.springer.com/article/10.1186/s40729-021-00346-7
- Cell-based therapies for alveolar bone and periodontal regeneration: a concise review. Stem Cells Transl Med. 2019;8:1286–1295. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6877771/
- First-in-human study and case reports of alveolar bone regeneration with the secretome from human mesenchymal stem cells. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4714459/











 70%
70% 
























































































































































































































































