

Dental implants are one of the most predictable treatments in dentistry — they survive in roughly 90–95% of cases over five years or more, so failure is uncommon.¹ But a small, real number do fail, and when they do it shows as a loose post, swelling, bleeding or discomfort that shouldn’t be there. The reassuring part is that most failures aren’t random: they follow recognised patterns, have identifiable causes, and a large share are preventable through careful planning before surgery and good care afterwards. This guide explains what failure actually means, the warning signs, every major cause (from peri-implantitis and smoking to diabetes and certain medications), whether a failing implant can be saved, and exactly how failure is prevented.
It’s the honest companion to the wider dental implant procedure — because understanding what can go wrong is precisely how a good clinic makes sure it doesn’t.
What “Implant Failure” Actually Means (and the Failure Rate)
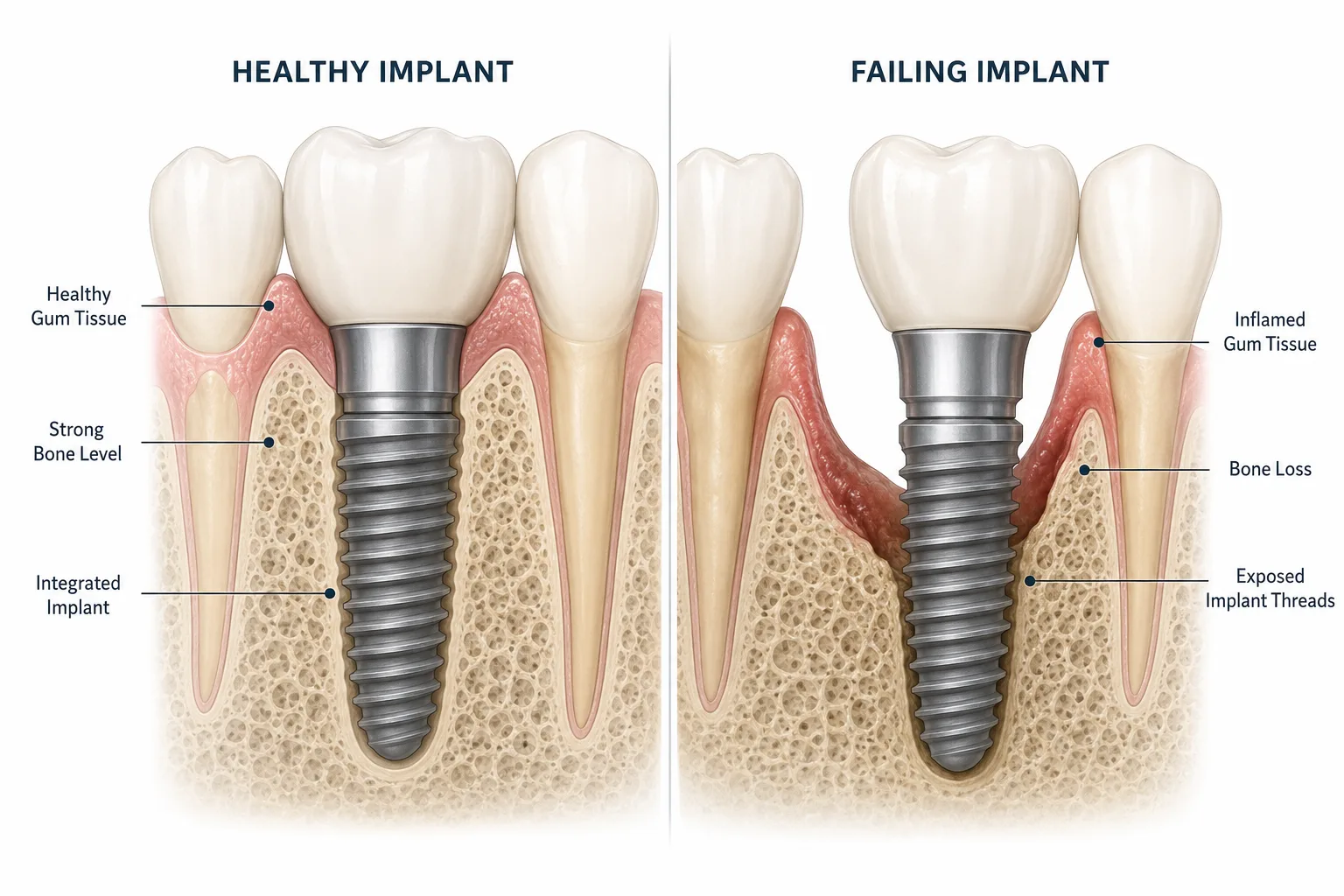
It helps to separate two ideas that often get blurred: survival and success. An implant has survived if it is still in the mouth and not mobile. It is a success if it has done that and the bone and gum around it are healthy, with no ongoing inflammation. An implant can technically survive while quietly failing — stable for now, but with bone loss or chronic inflammation building underneath. That distinction is why a good clinic tracks more than whether the implant is “still there.”
Failure in the strict sense is a breakdown of osseointegration — the implant does not fuse, or stops staying fused, with the jawbone it was meant to bond with. On the numbers, this is uncommon: long-term reviews put survival above 90% even after ten years, so failure sits broadly in the 5–10% range over the long term, with early surgical failure lower still.¹ When osseointegration truly breaks down, removal and a fresh start is usually cleaner than trying to rescue a post that never integrated — but caught early, many problems can be managed and the implant kept. Timing, as you’ll see, is the theme this whole article keeps returning to.
Early Failure vs Late Failure
Failures tend to cluster in two windows, and the causes differ in each.
- Early failure (first weeks to months), usually before or during osseointegration, traces back mostly to planning and surgery: poor angulation or positioning, bone density that was too low and wasn’t addressed first, infection soon after the procedure, not enough initial stability, or over-preparation of the implant site.
- Late failure (months or years later, e.g. after 5 or 10 years), after the implant has integrated and been working, traces back mostly to maintenance and biology: peri-implantitis, a misaligned bite or grinding, leftover cement below the gumline, poor hygiene, smoking, alcohol, uncontrolled health conditions, or a mechanical problem like a loose screw or chipped crown.
The pattern is worth remembering: early failures are mostly about planning and surgery; late failures are mostly about maintenance and biology. Both are addressable — just at different stages.
Warning Signs to Catch It Early
The single most important sign is movement — a healthy implant should feel as solid as bone, so any looseness of the implant or crown is often the first indication that integration is breaking down. Beyond that, see your dentist promptly if you notice:
- Persistent or returning pain around the implant, especially when biting or chewing.
- Swelling, redness or bleeding of the gum that lasts beyond the first couple of weeks, or any pus.
- Gum recession exposing the metal, a bad taste or smell, or the crown feeling lower than before.
- On an X-ray, visible loss of bone around the implant — the clearest objective sign your dentist will look for.
Mild swelling and soreness in the first few days is normal healing, not failure — here’s the realistic week-by-week recovery timeline so you can tell ordinary healing from a genuine red flag.
The Main Causes, in Plain Terms
Most failures come down to one or more of the following — and notice how many are within your or your dentist’s control.
- Peri-implantitis — the leading driver of late failure. This inflammatory infection of the gum and bone around the implant is common, affecting about one in five implant patients.² Daily cleaning and regular check-ups are the main defence; here’s how peri-implantitis is treated.
- Smoking — one of the biggest single risks. Implants fail more than twice as often in smokers as in non-smokers, because smoking impairs blood supply and bone healing.³
- Alcohol — heavy drinking, particularly during the healing phase, can interfere with bone metabolism and osseointegration, so limiting alcohol while the implant integrates is sensible.
- Uncontrolled diabetes — when blood sugar is poorly managed, healing and osseointegration are impaired and the risk of peri-implantitis and failure rises. Reassuringly, when diabetes is well controlled, implant success is comparable to non-diabetic patients.⁴
- Certain medications — some drugs affect bone metabolism. Antidepressants, particularly SSRIs, are associated with a meaningfully higher risk of implant failure (around twice the risk in pooled data),⁵ and bone-thinning medications used for osteoporosis can also be relevant. Always tell your dentist your full medication list.
- Bite overload & grinding (bruxism) — excessive force loosens the bond over time; a night guard often protects the implant.
- Insufficient bone at placement and poor oral hygiene — both avoidable with proper planning and aftercare.
Can a Failing Implant Be Saved?
Frequently, yes — if it’s caught early. Where the problem is infection, a thorough professional cleaning around the implant, sometimes with antibiotics or laser treatment, can settle peri-implant inflammation and stabilise the implant. Where the issue is the bite, an adjustment or a night guard relieves the overload. A loose screw or a chipped crown is usually a simple repair, because the restoration is removable.
If osseointegration has genuinely broken down, the cleaner route is to remove the implant, let the site heal — often with a bone graft to rebuild lost support — and place a fresh implant once the area is ready. The second implant has a high success rate when the original cause has been identified and corrected. The deciding factor, once again, is how early the problem is caught.
How Failure Is Prevented
Prevention maps neatly onto the two failure windows. Before surgery: plan from a 3D (CBCT) scan, treat any gum infection first, rebuild bone where it’s thin, review medications and health conditions, and place the implant with good primary stability. After surgery: clean around the implant daily, don’t smoke, limit alcohol while you heal, protect the bite if you grind, keep diabetes well controlled, and attend your check-ups so any early change is caught and reversed. Put simply, the assessment beforehand and the aftercare afterwards matter every bit as much as the surgery itself — which is exactly why they shouldn’t be an afterthought.
Frequently asked questions
What are the first signs of dental implant failure?
What is the failure rate of dental implants?
Do smoking, alcohol, diabetes or medications cause implant failure?
Can a failed dental implant be replaced?
Can dental implants fail after 10 years?
Why Patients Trust DentSpa for Implants
Because most failures are preventable, DentSpa plans every dental implant in Turkey from a 3D scan, reviews your health and medications, rebuilds bone where needed, and builds aftercare and remote support into the plan — the precise things that stop both early and late failure. If you’d like to understand the other side of longevity, here’s how long implants last and what extends their life. DentSpa was recognised as the Best Clinic in Dentistry in Europe at the European Awards in Medicine 2024 and has treated 50,000+ international patients. Book a free consultation to have your case planned properly from the start.
Sources
- 1. How far can we go? A 20-year meta-analysis of dental implant survival rates (~94.6%). PMC. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11416373/
- 2. What is the prevalence of peri-implantitis? Systematic review & meta-analysis (~1 in 5 patients). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9583568/
- 3. Smoking and dental implants: systematic review & meta-analysis (smokers fail >2× as often). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8780868/
- 4. Diabetes mellitus and dental implants: systematic review & meta-analysis (glycaemic control & failure). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9105616/
- 5. The effect of antidepressants on dental implant failure: systematic review & meta-analysis (raised risk ~2.4×). PubMed. https://pubmed.ncbi.nlm.nih.gov/38498803/











 70%
70% 
























































































































































































































































